By: Dr.Basam Abu Hamad
Health Consultant
Al-Quds University
Macro
context:
Historically,
the Palestinian people's right to control their lives and build their state was
denied and hindered by being successively and continuously under tutelage,
mandates and occupations. The consequences of this reality affected the social,
cultural, as well as the mental composition of the Palestinian people and
created a unique case of complex combination of challenges due to the burden of
the occupation, oppressions, economic disadvantages and socio-cultural
limitations. Unlike politically stable areas, occupied Palestinian territory
(oPt) in general and Gaza governorates in particular are witnessing an enormous
wide range of life challenges and suppressors. Palestinians didn’t enjoy
minimum level of viable stability required to establish coherent and concrete
system at which polices, regulations and services are consistent and
coordinated. This is true for the health system which spent most of time and
efforts as a fire fighter and seldom possessed the vision combined with ability
to act on a wider scope of protecting and promoting people's health and
wellbeing.
In
the last few years, the situation for more than 1.6 million Palestinians in the
GS became worse than it has ever been since the start of the Israeli occupation
in 1967. Occupation, conflict, siege, closures and the frequent wars have left
the high densely populated the GS in a state of severe vulnerability. The
current isolation has taken the humanitarian situation to an unprecedented
level, with coping mechanisms exhausted, widespread absolute poverty and an
inability of civil society organizations and formal authorities to meet even
the basic needs of the population. The collapse of the economy has left
little money to buy food, and little food in the local market to buy. The
ability of local communities to purchase required medicaments, contribute to
medical fees and pay for transport to reach health facilities is dramatically
decreasing (PNGO, 2009).
The
siege that “Israel” has intensified on the GS since June 2007 which continues
in a way or another till now have greatly harmed Gaza’s health system, which
had struggled even before these events. The severity of the situation has
increased exponentially since Israel imposed extreme restrictions on the
movement of goods and people in and out of Gaza in June 2007. Since then,
healthcare for people in Gaza has dramatically deteriorated at two levels; the
provision of health services inside Gaza and access to treatment outside Gaza.
Geographically:
The GS is a narrow band of land; it is 45 kilometres
long and 6-12 kilometres wide with an area of 378 square kilometres which has
suffered a lot from recurrent occupations. After the end of the First
World War, Palestine was placed under the British Mandate. The
GS was under the Egyptian Administration from 1948 to 1967, then it was
occupied by the Israeli Army in June 1967. The Israelis officially handed
the GS to the PA in 1994 according to the Oslo Agreement which was signed
between Israel and Palestinian Liberation Organization, in what was known as
"Declaration of Principles on Interim Self-Government Arrangements",
a document also known as the "Oslo Accords". The
implementation of the partial autonomy in 1994 and the establishment of the PA
have had its impacts on the society after the many devastating wars and the
long years of occupation and dispersion over the globe. However, still,
Israel holds overall sovereignty over the GS. It controls borders,
movement of goods and travellers, particularly the Gazans themselves. It
also controls trade, the commercial market, water, food, energy sources (fuel,
gas and electricity), the means of communications and the overall
security. Hence, it still has a hold over the local Palestinian economy.
The first turning point of the political and socioeconomic situation started to
deteriorate after the second uprising which sprang off in 2000 in the GS and
WB. A historical turning point occurred in June 2007 following the
"Hamas" takeover of the GS. Since then, a tight siege has been
imposed on the GS and the Israeli policy sought to ensure ‘no development, no
prosperity and no humanitarian crisis' (Oxfam, 2007; World Food Program et al,
2008; PNGO, 2009). The siege that Israel has intensified on the GS
since June 2007 has greatly harmed the health status and the health system,
which had struggled even before these events. However, signs of
humanitarian crisis are clearly obvious. The already insecure,
impoverished and imprisoned, Gazans have continued to live under dire
conditions. The Israeli government has stopped virtually everything
(except occasionally allowing some basic foodstuff and some medicines to enter
Gaza), as well as almost all citizens, from entering and leaving the GS.
Late in 2007, Israeli declared the GS a ‘hostile entity’. The Israeli
government subsequently reduced the supply of fuel and electricity to the GS
resulting in further destruction of the already exhausted economy and
distortion of basic services including health and sanitary services.
The
internal political division between the two main political parties “Fateh and
Hamas” in 2007 is also affecting the social and work values and systems, with
frequent disruptions of work and diminished productivity. Distortion of work
accountability system, disintegration of the social fabrics and work values and
the increase in the political partisan trend, are all among the negative
consequences of the division that have become the common norm in the
organizational environment. The loyalty then generally became to the ruling
party and not necessarily to the organizational objectives. An example of the
state of organizational lawlessness is the catastrophic behaviour of thousands
of MOH employees (still more than 2000 employees since 2008) have refrained
from their work, of those, many engage important technical and managerial
positions in the organization; they guaranteed that their salaries will be
continuously effused from the slush politicized funds, while they stay home.
Meanwhile, those who were committed to their jobs and kept covering their on
duty time, had their salaries cut.
In
22 days, December 27th 2008 through January 17th 2009, Israel
launched a large scale Israeli aggression on Gaza which resulted in thousands
of deaths and injuries among people and uncharitable damage of thousands of
houses, manufacture compounds, agricultural resources, drinking water and
sewage systems, government buildings, health facilities, electricity plant and
its networks. Most injuries were serious and strange in nature; often
multiple injuries, with head, thorax, abdominal and multi-limb injuries
(Ministry of Justice, 2009). Israel’s three-week military aggression
resulted in deaths of 1,455 people, of them, 553 (38%) were children and women;
and 5,380 people injured, of them, 2671 (49.6%) children and women, and massive
damage to dozens of thousands of homes, businesses, and infrastructure (Ministry
of Justice, 2009). In addition, during the period between November 14th through
November 21st 2012, “Israel” launched another military aggression on Gaza.
During the course of the operation, Israel struck more than 1,500 sites
in the GS, including government buildings, houses and apartment blocks and
institutions. MOH health information system database illustrates that 186
Palestinians died in the operation, with between 47 children and 13 women. An
additional 1,399 Palestinians were injured, and between hundreds of thousands
were displaced. Israeli strikes by air, land, and sea resulted in
civilian casualties, including those of children, in schools, soccer
fields and civilian residences.
Demographically:
Recent
reports indicate that the GS is among the most densely populated areas on
earth. According to the Palestinian Central Bureau of Statistics (PCBS),
the total number of the Palestinian population residing in the GS in mid-2012
is around 1.64 million (PCBS, 2012); the projected 2018 figure is around 2
million (PCBS 2012a; UN, 2012). The estimated number of annual deliveries
has increased from 50,000 deliveries in 2008, 53,000 in 2009, 60,000 in 2010
(MOH Field Statistics). However, it dropped in 2012 to around 56,000. Assuming
that the fertility rates will continue in the same trend, it is anticipated
that around 75,000 deliveries will be recorded in 2018 with more than 200
deliveries daily. The Palestinian population in Gaza has one of the
highest fertility rates in the region (around 5), compared to 3.8 in the WB,
3.5 in Egypt, 3 in Lebanon, 2.4 in Israel and 3.2 in Turkey (PCBS, 2012).
The crude birth rate in the GS in 2010 was 37.1 (PCBS, 2012) and the population
growth rate was 3.37% in 2011. Demographic trends anticipate that it will
slightly decline to 3% in 2018. Nevertheless, the crude death rate in the GS is
3.9 per 1000 population (MOH, 2012a).
The
inevitable increase in the population will pose further strains on access to
livelihood conditions of the Palestinians including housing, employment and
health services. Population growth and the high number of adolescents who will
enter the labour force in the coming years also mean that the health services
will have to grow in line, just to keep pace with the expanding.
Age
structure in the GS is similar to that in many developing countries, where
nearly half of the total population is under 14 years old (20% in UK).
Children under 5 years old represent around 18% (MOH, 2012a). In addition
to overall population growth, the fact that the GS has one of the youngest
populations worldwide will pose particular challenges. Some 51% of the
inhabitants are younger than 18 years, projected to decrease slightly to 48% by
2018 (UN, 2012). The GS has the second-highest share of people aged 0 to
14 years worldwide. Moreover, the ‘youth bulge’–the ratio of youth (15-29) to
the total over-15 population–is exceptionally high, at 53% (projected to
decrease to 52% in 2018). The life expectancy for males in Gaza is around 70
years and for females is 72.5 (PCBS, 2012). With the increase in the
expected life span, from 65 years in 1994 to 73 years in 2012 (according to MOH
reports), the elderly population aged 65 years and over constituted 2.4% of the
total population which has increased by five times in comparison to 10 years
ago (it is around 21% in Europe). It is anticipated that the proportion of
elderly people will increase with additional burden on the health system as
they are exposed to chronic diseases and require rehabilitation services.
The majority of households of the Palestinian population in the GS are nuclear
families (81%) with an increasing trend (PCBS, 2012). The reported
average family size is around 6.3 persons according to PCBS (2012a) with higher
rates at the North (6.7) and Rafah (6.5). Regarding housing
density, it was 1.8 per room in 2010, in 53.8% of households, 1 to 2
persons were living per each room, in 32.9% of households, more than 2 persons
were living in each room and in 13% of households more than three persons were
living in each room (PCBS, 2012). More than 71,000 housing units are currently
needed in Gaza (UN, 2012). The population density in the GS is more than
4500 inhabitants per one square kilometre in 2012 (PCBS, 2012) which is expected
to rise to 5500 in 2017. If we exclude the safety buffer zones near the green
line (accessibility is not allowed to Palestinians in these areas), the actual
population density will be much higher. Dependence ratio is estimated at
more than 80.5 for WB/G with higher ratio in Gaza (PCBS, 2012). According to
PCBS (2012), the literacy rate among Palestinians including females is high
(above 95%). Traditionally, Palestinians place a high value on education
and regard it as a durable and movable asset “contrary to land and houses that
can be and were lost”; therefore, this value is instilled in their children.
According to the PCBS (2012), the majority of the GS population are refugees
(66.1%) who receive basic primary health care services and some secondary care
services through UNRWA.
Households’
conditions:
The
recently released PCBS Report (2012) indicates that 40% of the households in
the GS were living in houses, 60% in apartments; with increasing trends.
The same source indicates that 93.6% of the households surveyed own their
residency place and 3.7% were living in rented houses. The survey
conducted by the Institute of Community and Public Health, Birzeit University
(ICPH-BU) in 2009 showed that 30.1% of households were using the public network
for obtaining drinking water, almost all households surveyed (99.8%) were
connected to the public electricity network and have had the basic
household assets such as refrigerators (93.7%), TVs (98.7%), Gaz for cooking
(95%), washing machines (96.2%) and basic furniture. Only 52% of houses
in Gaza have had computers at the household and 12% owned a car (PCBS,
2012). Around 23 areas in the GS are connected to the public sewage system
and 29 are using alternative methods such as septic tanks (PCBS, 2012).
In ordinary situation, 60% of households suffer from food insecurity or
potential for suffering from food insecurity. During the Israeli
aggression in 2008/2009, according to ICPH-BU, 2009 survey, food shortage were
reported by 80.9% of families during the war as a result of lack of food in the
market, lack of resources, restricted movement of goods and people (Israeli’s
shot on sight policy). According to the same source, shortage in drinking
water were reported by 69% of the households surveyed during the Israeli
aggression as a result of lack of electricity to pump water to households,
destruction of infrastructure and movement restriction of municipality.
Currently, 70% reported receiving food aid mainly through UNRWA and
international organizations. MOSA provides regular assistance to around 57,000
families; UNRWA supports 21,000 families and other organizations financially
support large number of families (MOSA field statistics). It could be
concluded that the livelihood safety network was not effective during the war
and people were starving. The availability of safety valve during emergency
situation is essential to ensure that basic livelihood conditions are
maintained. Emergency plans should be prepared to ensure that people have
access to essential items such as food and water during crises.
Environmental status:
Of
the 2000 water wells in the GS, 800 have stopped from work, of which many need
maintenance and rehabilitation to resume pumping water again (Addameer
Association for Human Rights, 2009). According to UN (2012) only
5-10% of the 150 water wells that cover the domestic water needs of the
population meet the international specification of safe drinking water in the
GS, while 40% meet the acceptable specifications of safe drinking water
according to the local standards. In 2010, the total water samples that were
chemically tested by the MOH laboratories, 73.5% did not comply with the local
accepted standards' specifications of safety of the drinking water (MAP and
Save the Children, 2012). A study conducted by the WHO showed that 30 of the
examined samples taken from the Gaza sea were contaminated with animal and
human faeces and an additional 25% are contaminated with animal faeces only
(WHO, 2008).
Electricity
outage is prominent for many years in Gaza especially during Israeli
aggressions. In June 2006, Israel destroyed the main power plant in Gaza after
the kidnapping of “Gilat Shalet”. Since then, mass punishment measures
have been enforced on the inhabitants living in Gaza till now. Currently, at
least, there is electricity cut for 8 hrs a day which could increase to 12 hrs
in ordinary situation. The current capacity for electricity supply is 242
MW. The demand in 2011 was 350 which is expected to rise to around 550 in
MW 2018 (UN, 2012). Other environmental challenges include air and
soil pollution, desertification, scarcity andsalination of fresh
water, sewage treatment, water-borne diseases, soil degradation,
poor solid waste management and depletion and contamination of underground
water.
Economical
context :
The Gross Domestic Product (GDP) in the GS could not be traced reliably from
local sources because of the chaos political situation as described above,
however, it was estimated at $ USA 1.3 billion in 2003, and declined to 1.1
billion in 2008 although the population has increased by around 30% during that
period (PCBS, 2010). The annual GDP for Gaza per capita in 2008 was $
774.5 which is less than 40% of that of the WB figure (1,718.4) (PCBS,
2010). It seems that it has increased to $ 1156 in 2011 and is
expected to reach $ 1273 in 2015 (UN, 2012). The average monthly
household expenditure and consumption in Dinar (JD) in GS Governorates, in 2010
is around 670 (PCBS, 2012). The main sources of livelihood in Gaza are
employment at the services sector (mainly at government, UNRWA and NGOs),
rain-fed agriculture, livestock rearing and fishing (PCBS, 2012).
According to the PCBS Report (2012), the percentage of those who are older than
15 years in labour force is 40.2% and 59.8% were outside the labour
force. The same source indicates that among those in labour force, 56.3%
were employed and the rest 43.7% were unemployed.
To
conclude, this combination of economic and social deterioration, and the
inability of health services to respond to the consequences, has exacerbated
the already dire health status of the population of Gaza. Any kind of economic
recovery in Gaza is impossible while the blockade of Gaza remains in place.
Even if it is lifted, it will take years to repair the damage and to recover
the economy. More aid is going to the Palestinians than before and yet the
humanitarian situation continues to decline. Continued aid is vital to respond
to the growing humanitarian crisis in Gaza but it cannot provide a solution in
itself. Consequences of the above situations imply that urgent measures need to
be taken to support the delivery of health services and to meet the increasing
demands for health services particularly for mothers, children, elderly, PWD
and sick who are more vulnerable than other groups. The demographic characters
of the Gaza population imply that there is an increasing load on the health
sector, particularly Mother Child Health (MCH) services and NCD which affect
older population. The health system should respond not only to the
current contextual challenges, but also to the increasing demands for services
resulted from increased population size. Therefore, planners, policy makers and
donors need to consider these factors in a manner that meets current and future
needs of the Gaza population.
General health status
of the population:
Compared
to other countries at a similar level of economic development, the Palestinian
population’s overall health status outcomes are relatively good partially due
to the strong performance on most basic public health and PHC functions (PNGO,
2009). Women education, family commitment and cultural values are also
important factors in this regard. Also political commitment to health is
obvious as manifested in high spending on health around 9-12% of the GDP which
has recently increased and reached more than 15% (PCBS and MOH, 2011); OECD
(2012) figure is (9.5%) of the GDP. Spending on health per capita has
increased from $ 120 (1994) to $ 165 in 2008 (OECD figure in 2012 was $ 2377;
Jordan $ 238; Syria, $ 100; Egypt $ 38).
Given
the prevailing complexity health sector in general face; lack of resources,
blockade, siege, uncertainty, the heavy consequences of political division
among the Palestinian parties, and expanding needs of people, maintaining
service provision to citizens is a credit recorded to the Palestinian health
sector. It is worth mentioning that the health sector exerted significant
efforts not only to maintain health services but also to improve and present
some new services such as opening of a new specialized services at MOH premises
such as cardiac surgery and cardiac catheterization, introducing new schemes
for health services such as Family Medicine by UNRWA, maintaining adequate
coverage of rehabilitation services by the NGO sector and maintaining most of
the achievements made by the health sector. Among the issues that the
health sector should be acknowledged for is the heavy investment in IT, HIS,
training and developing human resources in some sub-specialties.
Generally
speaking, healthcare services were effective especially when comparing health
outcomes in Gaza to those in the region. This is typically true regarding
mortality indicators, Infant Mortality Rate (IMR), Maternal Mortality Rate
(MMR), immunization coverage, causes of adults’ deaths and so on. Physical
access to services is generally acceptable in ordinary situation but it is
usually impaired during emergency situations. Most basic services are
satisfactory in terms of coverage and physical accessibility while the quality
of care is questionable due to lack of appropriate standards and weak
implementation of the already available ones. Also, access to advanced tertiary
services remains a real challenge facing the health care system in Gaza.
Although
the control of infectious diseases has been maintained with no reports of fatal
vaccine controllable diseases; still meningitis, hepatitis, diarrhoea and
others are common with high morbidity rates. Gaza is going through what
is called “epidemiological transition” with a shift from communicable diseases
to no-communicable ones with higher rates of heart diseases, hypertension,
diabetes and cancer. Non-communicable diseases including heart diseases,
cancer, hypertension and cardiovascular diseases and diabetes mellitus, are
gradually replacing the traditional enemies of infectious diseases as the
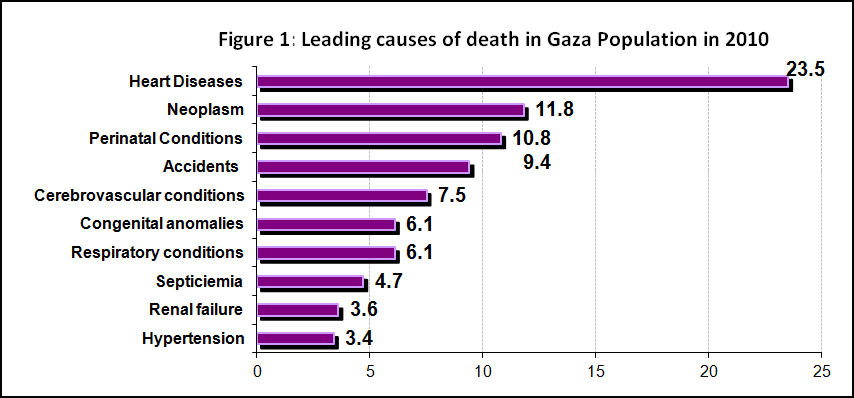
leading causes of death. Recent health reports (MOH, 2012a) indicate that only
4.7% of all deaths were reported due to infectious diseases/septicaemia.
Instead, the leading causes of death are chronic conditions, namely heart
diseases (23.5%), cancer (11.8%), perinatal conditions (10.8%), and
cerebro-vascular conditions (7.5%). In addition, all kinds of accidents
(intentional and un-intentional) accounted for 9.4% of deaths. Despite the limitations
in documenting root causes of death, this list constitutes a guiding frame for
strategic intervention.
Life
expectancy at birth level has reached to 70-71 years (79.8 in OECD) in oPt
(PCBS, 2012). Crude death rate remains constant at around 3.1 per 1000
population. Mortality indicators including IMR and MMR are within the
acceptable level, however, it didn’t improve as reported in most
countries. Almost all deliveries are institutionalized and attended by
skilful birth attendants. Anaemia and chronic malnutrition still
constitute public health problems especially among children and pregnant
women. Around 40% of males' youth in Gaza are smoking according to PCBS
report (2012a) (25.9% in OECD).
What
complicates the situation more is that the Palestinian community is suffering
from poverty-related diseases and illnesses, such as malnutrition, anaemia and
sanitary related diseases which have been aggravated due to conditions
associated with the current closure resulted in the deterioration of the sanitary
conditions. Nutrition problems are chronic in Gaza and cultural norms are a
contributing factor to this problem. Nutritional problems can be partially
alleviated by strengthening the ability of communities to advocate and support
appropriate nutrition practices. The knowledge of what healthy foods
constitute, appropriate eating habits, cooking practices, food storage and
possible food alternatives, are all important areas for nutritional awareness.
Anaemia preventive practices, such as drinking tea, consuming iron rich food
and consuming food rich in vitamin C constitute priority areas.